Encouraging Hair Growth by Reducing Senescence
In Aging Cell, researchers have described how to improve the hair growth potential of stem cells and organoids by reducing cellular senescence.
The quest for a true stem cell hair treatment
There has been a substantial amount of previous work in restoring hair follicle growth by culturing dermal papilla cells (DPs), which are the mesenchymal stem cells (MSCs) responsible for hair growth within follicles [1]. However, utilizing these cells to treat patients has proved unexpectedly difficult: outside the context of an active hair follicle, these cells quickly forget what they’re supposed to do and their hair growing ability swiftly declines [2].
Furthermore, unlike with rodent cells, repeated passages of human DPs cause them to lose potency. While there have been multiple attempts to restore this through various methods, such as conditioned media [3] and implantation into an extracellular matrix [4], such approaches have only been documented to work on early-passage cells.
The researchers attribute some of this decreasing capability to a rise in cellular senescence, as senescent cells and their secreted compounds (SASP) have been listed as causes of dysfunction [5] and removing them has restored hair in a mouse model [6]. In a living animal, senescent cells are naturally cleared, such as by the immune system; however, this mechanism doesn’t exist in cell cultures.
Hair cells become senescent quickly in culture
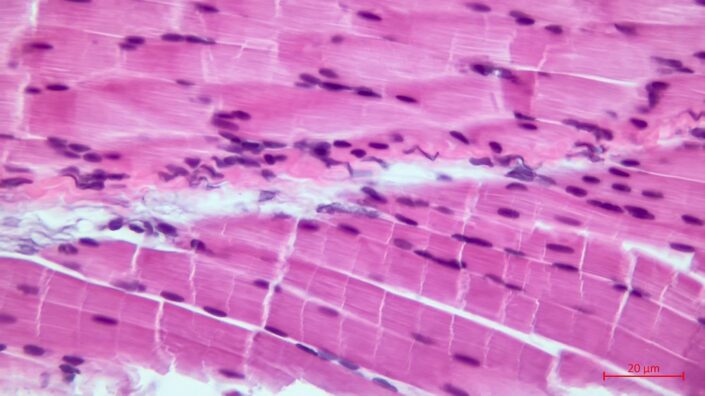
In their first experiment, the researchers extracted and cultured DPs and dermal fibroblasts (DFs) from the same donor. While those cells don’t grow hair, they are well-studied in the context of senescence and share a common progenitor with DPs.
The DPs rapidly became more senescent than the DFs, even from the very first cellular passage, according to the well-known biomarker SA-β-Gal. The DPs also rapidly became senescent according to several other markers, including a loss of proliferation and an increase in p16 and p21.
The rapid predominance of senescent cells in DP culture also meant a sharp increase in SASP factors, including the inflammatory factors IL-6 and IL-8. Compounding the problem, cells that were exposed to these inflammatory factors were found to have their own productive abilities suppressed. An RNA analysis confirmed these findings, showing a marked rise in SASP-related signaling among these cultured cells.
A senolytic solution
Senolytics, drugs that remove and destroy senescent cells, may or may not be advisable for living organisms, as senescence is required in some situations. However, in cell cultures, none of those concerns apply.
At passage 3, the researchers administered dasatinib and quercetin, a well-studied senolytic combination, to a population of DPs. This approach was effective: the senescent cells were rapidly killed off. Interestingly, many of the remaining cells entered into a quiescent state, as measured by the biomarker p27; however, quiescent DPs can be woken up and encouraged to fulfill their function, while senescent DPs cannot. As expected, senolytic treatment also removed the influence of the SASP, significantly reducing such SASP factors as IL-6 and the downstream effects.
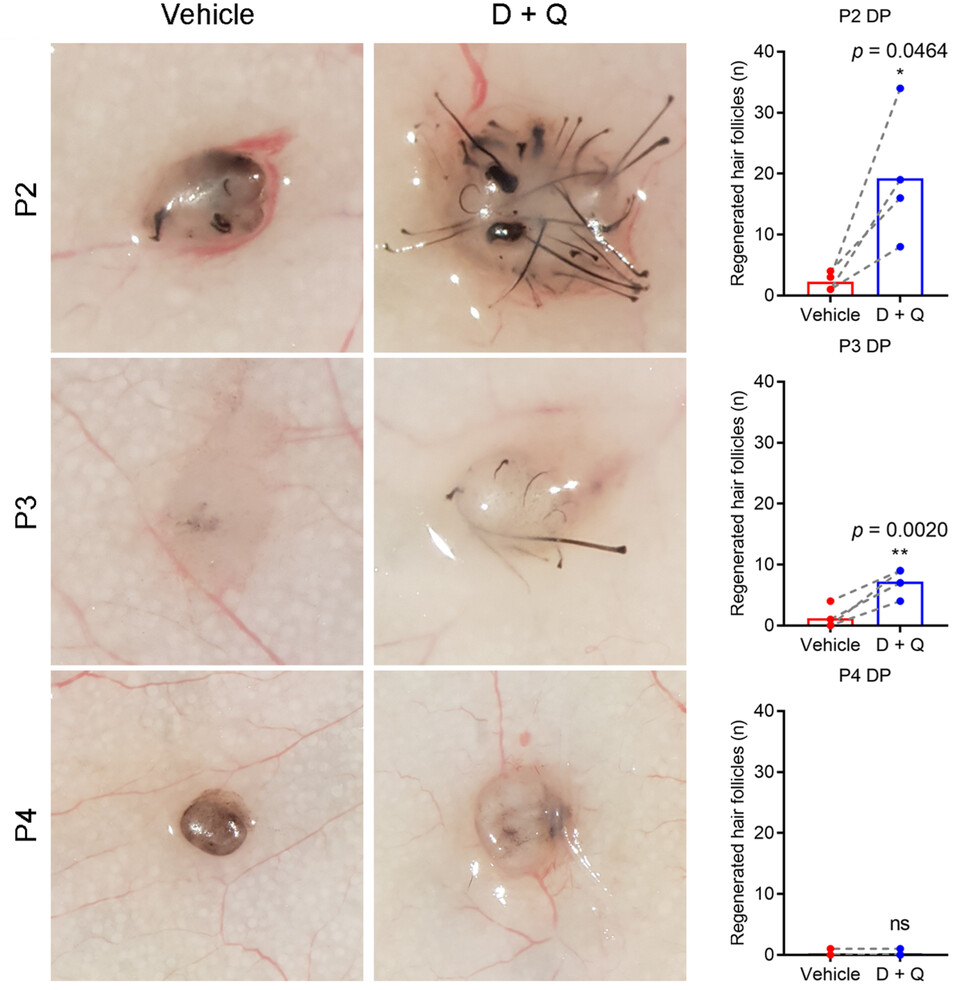
Intrigued, the researchers continued their work by first applying senolytics to DPs at passages 2, 3, and 4, and then using them to create 500 spheroids that each contained 2000 human DPs and a million mouse keratinocytes. They then implanted these spheroids into the backs of hairless mice. Compared to a non-senolytic control group, the senolytic-applied DPs were far more effective at growing hair. Unfortunately but expectedly, the DPs that were taken at passage 2 were more effective than similar cells taken at passages 3 and 4, demonstrating that while senolytics are effective, they are not a complete solution for later-passage DPs.
These results were recapitulated in an experiment involving cultured human skin. A million human DPs and two million human DFs were seeded in wells of collagen. The cells that were exposed to senolytics were found to grow keratin and hair follicle structures, but the control group that had not been exposed to senolytics did not.
While the researchers acknowledge that their work is incomplete and that they still do not have a readily available treatment for hair loss, they hold that senolytics are key in overcoming one of the major hurdles associated with this line of work. Further research will need to be done to create artificial human skin that can grow hair in the same way that the skin of living, healthy people can.
Literature
[1] Leirós, G. J., Kusinsky, A. G., Drago, H., Bossi, S., Sturla, F., Castellanos, M. L., … & Balañá, M. E. (2014). Dermal papilla cells improve the wound healing process and generate hair bud-like structures in grafted skin substitutes using hair follicle stem cells. Stem cells translational medicine, 3(10), 1209-1219.
[2] Ohyama, M., Kobayashi, T., Sasaki, T., Shimizu, A., & Amagai, M. (2012). Restoration of the intrinsic properties of human dermal papilla in vitro. Journal of Cell Science, 125(17), 4114-4125.
[3] Abreu, C. M., Cerqueira, M. T., Pirraco, R. P., Gasperini, L., Reis, R. L., & Marques, A. P. (2021). Rescuing key native traits in cultured dermal papilla cells for human hair regeneration. Journal of Advanced Research, 30, 103-112.
[4] Liu, Z., Huang, J., Kang, D., Zhou, Y., Du, L., Qu, Q., … & Miao, Y. (2023). Microenvironmental reprogramming of human dermal papilla cells for hair follicle tissue engineering. Acta Biomaterialia, 165, 31-49.
[5] Shin, W., Rosin, N. L., Sparks, H., Sinha, S., Rahmani, W., Sharma, N., … & Biernaskie, J. (2020). Dysfunction of hair follicle mesenchymal progenitors contributes to age-associated hair loss. Developmental cell, 53(2), 185-198.
[6] Baar, M. P., Brandt, R. M., Putavet, D. A., Klein, J. D., Derks, K. W., Bourgeois, B. R., … & de Keizer, P. L. (2017). Targeted apoptosis of senescent cells restores tissue homeostasis in response to chemotoxicity and aging. Cell, 169(1), 132-147.