A team of reviewers has taken a look at the relationship between cancer, cellular senescence, and vascular overgrowth and published this information in Aging Cell.
Different gut cancers form through different pathways
The authors begin their paper by discussing two cancers that are downstream of inflammatory bowel disease (IBD): colorectal cancer (CRC) [1] and colitis-associated cancer (CAC) [2], which is the focus of this review. These two cancers are similar but have key distinctions: sporadic CRC follows an adenoma-carcinoma transition, while CAC goes from inflammation to dysplasia to cancer [3]. In CRC, mutations to tumor suppressor 53 (TP53) happen later on, but in CAC, these mutations occur earlier, and other cancer-related mutations happen later than in CRC [4]. This review suggests that such distinctions “support the view that chronic mucosal inflammation imposes a distinct evolutionary pressure on intestinal tumorigenesis.”
The reviewers also note that aging and senescence are also playing roles in these conditions. Aging, in addition to harming the genome, changes the microenvironment of the gut in various ways that promotes cancer [5]. The increasing numbers of senescent cells also affect this microenvironment, increasing inflammation while increasing fibrosis and generating more blood vessels (angiogenesis) [6], which is associated with cancer growth [7].
Normally, this excess of blood vessels is governed by vascular endothelial growth factor (VEGF), so treatments are designed to reduce it. However, VEGF-centered treatments may not be particularly effective against angiogenesis in CAC, which is supported by a “broad and more redundant” collection of factors that are caused by inflammation and injury [8]. This includes the senescence-associated secretory phenotype (SASP) [9].
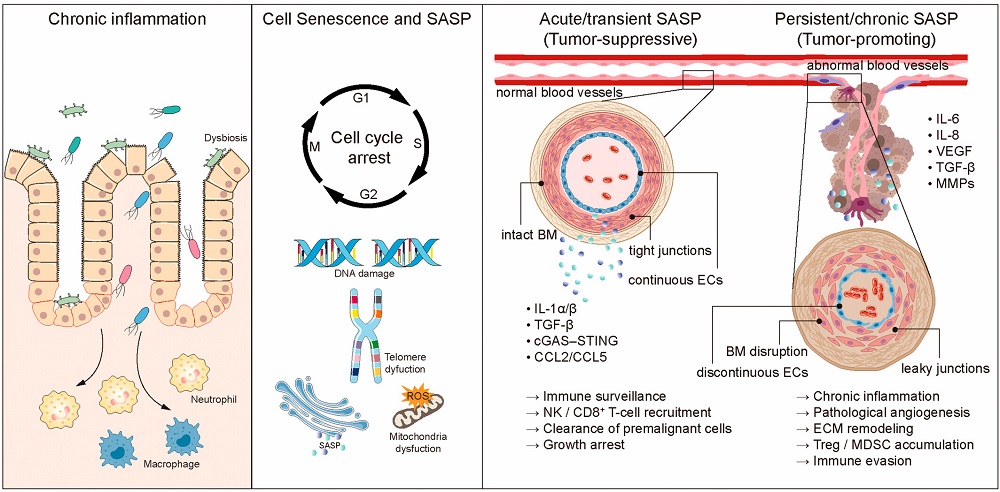
Cells can be driven senescent in a variety of ways, but in IBD, many of the offending cells have undergone stress-induced premature senescence (SIPS), which occurs when genetic damage, oxidative stress, and inflammation become sufficient to cause cells to stop replicating [10]. While senescence itself can be protective against cancer, the inflammation caused by the SASP is well-known to have the opposite effect. There appear to be few, if any, significant differences between the SASP in other conditions and the SASP in IBD; the reviewers list many of the well-known inflammatory cytokines, chemokines, and matrix remodeling proteins that are frequently secreted by these cells.
The SASP causes malformed blood vessels to sprout
Within this context, the SASP affects two critical cellular types in addition to immune cells. Epithelial cells, which line the intestines, normally form crypts where their stem cells proliferate; murine experiments have found that inflammation distorts these crypts and induces senescence in these once-proliferating cells [11]. Stromal cells, which form connective tissue, are driven to fibrosis and pathological angiogenesis when exposed to the SASP [12]. The persistent inflammation of the SASP also exhausts immune cells [13], depriving them of their ability to perform critical functions – such as clearing senescent cells.
The SASP factors involved in angiogenesis have been identified. Specifically, the well-known inflammatory factor NF-κB drives IL-6 and IL-8 production, while IL-6 drives JAK/STAT3 signals that, in turn, increase MMP-9 and VEGF [14]. The researchers explain that this SASP signaling causes both injury and misguided repair mechanisms, thus remodeling the tissue microenvironment in a negative way.
The blood vessels that are created by SASP-induced angiogenesis are, themselves, unhealthy. They are structurally unstable with poorly maintained endothelial junctions, and immune cells do not proceed normally through them [15]. This endothelial malfunction causes the production of various immunosuppressive factors while preventing the entrance of cells that would normally kill abnormal cells [16]. Unsurprisingly, this provides an ideal environment for cancer to grow, so the reviewers hold that pathological angiogenesis is not just a side effect of IBD but a core reason why it contributes to cancers such as CAC.
What can be done about it?
The reviewers list a wide variety of senolytic and senomorphic drugs as potential methods for dealing with the SASP’s effects in IBD. However, not all senescence is negative in this context; the reviewers also note that persistent senescence is different from acute senescence, which may be protective against tumors. Reducing angiogenesis has been found to induce senescence in cancer cells themselves [17]. The reviewers recommend attempting to combine senolytic or senomorphic treatments with anti-VEGF therapies. In the future, they hold that “precision interventions may emerge to prevent colitis-associated neoplasia and improve long-term outcomes in IBD.”
Literature
[1] Liu, D., Cao, M., Wang, H., Cao, W., Zheng, C., Li, Y., & Wang, Y. (2024). Association between inflammatory bowel disease and cancer risk: evidence triangulation from genetic correlation, Mendelian randomization, and colocalization analyses across East Asian and European populations. BMC medicine, 22(1), 137.
[2] Li, J., Ji, Y., Chen, N., Dai, L., & Deng, H. (2023). Colitis-associated carcinogenesis: crosstalk between tumors, immune cells and gut microbiota. Cell & Bioscience, 13(1), 194.
[3] Carethers, J. M., & Jung, B. H. (2015). Genetics and genetic biomarkers in sporadic colorectal cancer. Gastroenterology, 149(5), 1177-1190.
[4] Rajamäki, K., Taira, A., Katainen, R., Välimäki, N., Kuosmanen, A., Plaketti, R. M., … & Aaltonen, L. A. (2021). Genetic and epigenetic characteristics of inflammatory bowel disease–associated colorectal cancer. Gastroenterology, 161(2), 592-607.
[5] Fane, M., & Weeraratna, A. T. (2020). How the ageing microenvironment influences tumour progression. Nature Reviews Cancer, 20(2), 89-106.
[6] Gorgoulis, V., Adams, P. D., Alimonti, A., Bennett, D. C., Bischof, O., Bishop, C., … & Demaria, M. (2019). Cellular senescence: defining a path forward. Cell, 179(4), 813-827.
[7] Senga, S. S., & Grose, R. P. (2021). Hallmarks of cancer—the new testament. Open Biol 11: 200358.
[8] Francescone, R., Hou, V., & Grivennikov, S. I. (2015). Cytokines, IBD, and colitis-associated cancer. Inflammatory bowel diseases, 21(2), 409-418.
[9] Chambers, C. R., Ritchie, S., Pereira, B. A., & Timpson, P. (2021). Overcoming the senescence‐associated secretory phenotype (SASP): a complex mechanism of resistance in the treatment of cancer. Molecular oncology, 15(12), 3242-3255.
[10] Dierick, J. F., Eliaers, F., Remacle, J., Raes, M., Fey, S. J., Larsen, P. M., & Toussaint, O. (2002). Stress-induced premature senescence and replicative senescence are different phenotypes, proteomic evidence. Biochemical pharmacology, 64(5-6), 1011-1017.
[11] Lopetuso, L. R., Murgiano, M., Mantuano, E., Schiavone, V., Costa, A., Mascianà, G., … & Costa, G. (2025). The Molecular Landscape of Inflammation in Inflammatory Bowel Disease (IBD): Targets for Precision Medicine. Biomedicines, 13(11), 2738.
[12] Rieder, F., Mukherjee, P. K., Massey, W. J., Wang, Y., & Fiocchi, C. (2024). Fibrosis in IBD: from pathogenesis to therapeutic targets. Gut, 73(5), 854-866.
[13] Wu, Y., Wu, Y., Gao, Z., Yu, W., Zhang, L., & Zhou, F. (2026). Revitalizing T cells: breakthroughs and challenges in overcoming T cell exhaustion. Signal transduction and targeted therapy, 11(1), 2.
[14] Li, Z., Zeng, L., Huang, W., Zhang, X., Zhang, L., & Xie, Q. (2025). Angiogenic factors and inflammatory bowel diseases. Biomedicines, 13(5), 1154.
[15] Dudley, A. C., & Griffioen, A. W. (2023). Pathological angiogenesis: mechanisms and therapeutic strategies. Angiogenesis, 26(3), 313-347.
[16] He, S., Zheng, L., & Qi, C. (2025). Myeloid-derived suppressor cells (MDSCs) in the tumor microenvironment and their targeting in cancer therapy. Molecular cancer, 24(1), 5.
[17] Foersch, S., Sperka, T., Lindner, C., Taut, A., Rudolph, K. L., Breier, G., … & Waldner, M. J. (2015). VEGFR2 signaling prevents colorectal cancer cell senescence to promote tumorigenesis in mice with colitis. Gastroenterology, 149(1), 177-189.